
The Joint By Joint Approach and Why It Matters
Today we’re going to talk about Mike Boyle’s joint-by-joint approach that was featured in his book Advances in Functional Training. This model shows how the function of joints can have effects all the way up the kinetic chain, both good and bad. Today, we’re going to talk about this model, and specifically why you should just say “no” when it comes to using preventative ankle tape.
Before We Get Started
Before we get going here I want to clear up a few things. When it comes to recovery and injury prevention modalities I’m on the fence with a lot of them. I’m not a fan of ice, and I did a podcast episode about it a few years back (it’s one of the first episodes I ever did, so it’s a little bit rough but there’s good info in the episode). I’m not a huge fan of many of the modalities used in the training room as the evidence that it’s effective is sparse, and my modalities professor in college turned me off to many of them. The takeaway from Modalities in College was “if it works in the athlete’s mind, then it works, but they don’t actually work.” That being said, if you feel like they work then they work and I would say to continue to use them. However, using ice (and NSAIDs) and preventative ankle tape is where I draw the line because they’re counterintuitive to their use. We’ll talk about the “why” now.
The Joint By Joint Approach
The body is a series of joints stacked on top of each other. Each joint has its own function, and if that function becomes impaired then the system ceases to work the way it’s supposed to. The way each joint functions, affects the joint both above and below it.
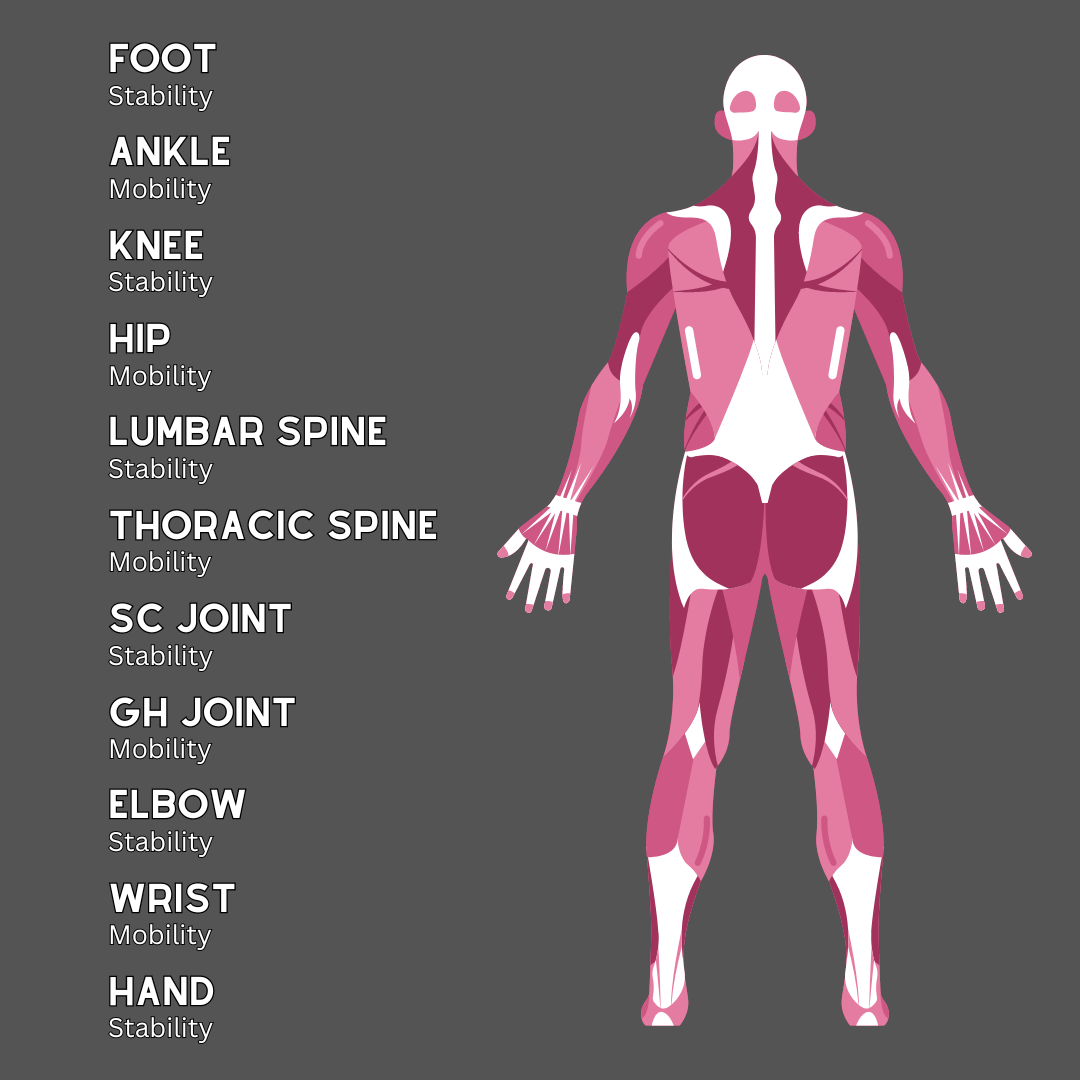
These joints that are stacked on top of each other alternate in their functionality. These functions are mobility and stability at every major joint. This is a graphic showing the functions of each joint, starting at the foot and going all the way up the kinetic chain to the hands.
Foot - Stability
The foot is a very stable joint. We’re not talking about your ankle joint, but the actual joints within the foot. You’ve probably never thought about it, but if you try to move your foot outside of curling and extending your toes right now you’re going to find out there isn’t much movement. You could say that the “foot joint” flexes and extends while not offering much else in the way of movement.
This joint is stable because every action we take involves driving force through this joint and into the ground. From walking to sprinting and jumping and even standing, the foot takes a beating. If the foot was not a stable joint, then we would not be very efficient movers and we’d be susceptible to injury quite often.
Ankle - Mobility
The ankle is a very mobile joint. The ankle performs the following actions:
Flexion (plantarflexion)
Extension (dorsiflexion)
Eversion (pronation)
Inversion (supination)
Circumduction
The ankle can move in all planes of motion and is designed to allow our knee and hip joints to perform their jobs efficiently. We also have the added bonus of the heel cord crossing the ankle joint which is what allows us to sprint and jump with elasticity. If the ankle were not incredibly mobile, it would be almost impossible to move from side to side. The mobility of our ankle allows for stability at both the knee and the foot.
Knee - Stability
The knee joint is a very stable hinge joint. The main actions of the knee are:
Flexion
Extension
Although there is also some internal and external rotation at the tibia, it’s minute and not considered one of the main functions of the knee. The knee can also abduct and adduct very minimally as well. This joint is a major force creator/transferer, which is why we need a lot of stability in this joint.
Hip Joint - Mobility
The hip joint is supposed to be very mobile. That isn’t always the case with us today because we sit for so much of the day, everyone specializes in incredibly movement skill-specific sports, and we play the same sport all year long. The hip joint is a ball-and-socket joint and performs the following actions:
Flexion
Extension
Abduction
Adduction
Internal/External Rotation
Circumduction
The hip joint allows for stability in the lumbar spine and the knee. The hips help balance our torso as we go through any kind of movement, and this mobility quite literally allows us to move.
Lumbar Spine - Stability
The lumbar spine is a joint that has minimal movement. There is some rotation, but the majority of the movement in your lumbar spine is flexion and extension, along with some lateral flexion. There is some rotation, but it isn’t one of its main functions. A ton of force runs through the spine, particularly the lumbar spine and this stability helps to protect our spinal cord from injury.
If you’ve ever heard that you shouldn’t use a foam roller on your lower back, this is why. That tightness you sometimes get in your lower back when you exercise (or sit a bunch) is a protective mechanism. We’ll go into depth about why this happens later in this article.
Thoracic Spine - Mobility
The thoracic spine is the middle and upper part of your back. There are 12 thoracic vertebrae, and they sit between the cervical spine and the lumbar spine. This area of your spine is designed for mobility, however, it’s a weird “joint” (really 13 joints) since it’s relatively stable due to the ribcage that it attaches to. The thoracic spine vertebrae can perform the following actions:
Rotate
Flex
Extend
Lateral flexion
Thoracic mobility is typically lost in society today due to the amount of sitting that we do, and more recently the amount of looking down at our smartphones that we do throughout the day as well. We end up with a kyphotic posture in our thoracic spine and lose the mobility we need. When this happens we’ll gain it in places we don’t want mobility.
Scapulothoracic (SC) Joint - Stability
The SC joint isn’t technically a joint, but it functions like one. The SC joint, much like the lumbar spine, needs some level of mobility however, it needs to maintain stability for our shoulder joint to function the way we need it to. The SC joint does the following:
Elevation/Depression
Protraction/Retraction
Medial/Lateral Rotation
Most of the stability in the SC joint is created by musculature. There are a few ligaments that help to keep it in place, but like I said it’s not really a joint in the sense that the rest of the joints we’ve talked about are. Rotator cuff muscles and scapular stabilizers create the majority of the stability in this joint, which is why an overly kyphotic thoracic spine can lead to too much mobility in our SC joint, which we do not want.
Glenohumeral Joint (Shoulder) - Mobility
You can think of the GH joint as the hip of the upper body. It is a ball-and-socket joint that has many functions. It functions in the following ways:
Flexion
Extension
Abduction
Adduction
Internal/External Rotation
Circumduction
The mobility at this joint allows for stability at the elbow and the SC joints, which is incredibly important for both life and sports in general. While mobility is important, we also need to maintain some level of stability for this joint to function properly, and that stability is created by the rotator cuff and believe it or not, scapular stability.
Elbow Joint - Stability
The elbow is much like the knee of the upper body. The main difference is that there is a little bit more “internal and external rotation” that we call pronation and supination. The main joint actions of the elbow are the following:
Flexion
Extension
Supination
Pronation
The elbow also goes through what we call abduction and adduction, but it is very minimal. In fact, too much abduction tends to lead to UCL tears, leading to Tommy John surgery in a lot of overhead throwers. When the shoulder lacks mobility your body will find it in the elbow. The elbow joint is considered a stable joint.
Wrist - Mobility
The wrist is the ankle of the upper extremity. It’s incredibly mobile and this mobility is one of the reasons that we’re able to pick things up and throw things with accuracy. Wrist joint actions are the following:
Flexion
Extension
Abduction
Adduction
Circumduction
The wrist can move in all directions just like the ankle. This mobility allows both the elbow and the hand to perform its job safely and efficiently.
Hand - Stability
The last joint on this list is the hand joint and it is the foot joint of the upper extremity. While we don’t have the same level of force transfer in the upper body, the hand being stable allows us to pick up, hold, and throw objects with the forces we produce in our core, shoulders, and elbows. The hand joint performs the following actions:
Flexion
Extension
The hand “flexes” and “extends” but cannot really perform these actions on its own. Making a closed fist or opening up your hand mostly happens at the wrist and fingers, while the hand itself stays relatively stable throughout these movements. There are intrinsic muscles in the hand just like there are in the feet, and these are the muscles that allow for these small movements in the hand joint.
So Why Can’t We Use Ankle Tape?
I said at the beginning of this article that I’m not a fan of preventative ankle tape, and the reason for this is that it takes a very mobile joint, and makes it very stable. Movement is a series of muscle and joint actions that are all performed in unison and changing the way a joint functions (and such an important joint when it comes to movement at that) is going to change the way the system functions as a whole. I’ll give you an example below:
When you go to change directions laterally, there are a myriad of joint actions that take place. Here is a list of the big ones that take place during the first phase (when you slow down):
Hip - flexion and external rotation
Knee - flexion
Ankle - dorsiflexion and eversion
Lumbar spine - extension and some rotation
Thoracic spine - extension and rotation
When you take off out of that bottom position, you mostly perform the opposite actions:
Hip - extension and external rotation
Knee - extension
Ankle - plantar flexion and some inversion
Lumbar spine - stays extended
Thoracic spine - stays in extension and a little bit of rotation
Ankle tape puts your ankle into forced dorsiflexion and eversion/pronation. When we’re put into that position at the ankle, it causes valgus stress at the knee and also causes the hip to internally rotate. Add in the high forces of changing direction (upwards of 3-5x body weight), and you’re looking at the number one mechanism of injury for noncontact ACL and MCL tears (and meniscus tears as well).
Compensatory Movement
When your body performs movements, it will compensate in various areas to ensure the movement can be performed if there is a lack of mobility at any given mobile joint. Here are a couple of examples:
Can’t supinate/invert at the ankle to change directions? Your body will internally rotate at the hip so that you can create the proper angle.
Can’t externally rotate your shoulder enough to throw a ball? Your body will abduct at the elbow to create that angle.
Can’t flex your hip enough to get into a deep squat? We’ll flex in the lumbar spine to achieve squat depth.
There are a ton of other examples but these tend to happen the most often. We lose mobility in our hips, so we gain it in our lumbar spine and at the knee. This is why some people are under the impression that the squat and deadlift are bad for your back and knees. In reality, they’re great for both joints, but your body isn’t ready to squat yet because you lack the requisite mobility to accomplish the movement pattern.
When we lose mobility in our shoulders, our bodies will compensate by creating mobility in the SC joint, and worse, at the elbow. This is one of the reasons we have had an epidemic of UCL tears leading to Tommy John surgery in TEENAGE baseball players.
When we lose mobility in our thoracic spine, we gain it in our SC joint (and lumbar spine) which causes more stability in the shoulder (GH) joint. This is why sitting at a desk all day can eventually lead to some pretty serious shoulder pain. We become internally rotated at the shoulder, and protracted at the SC joint.
I’ve written previously about lower cross syndrome in the past, and that article is a really good read if you’re trying to pinpoint your lower back pain and how to fix it. Our bodies are great at adaptation which is great. But, it can also be a really bad thing when you start to lose mobility at joints that are meant to be incredibly mobile.
Putting it All Together
Understanding the joint-by-joint approach is incredibly important to understanding how your body operates, and if you’re a personal trainer or strength and conditioning coach it should be the basis of your movement selection for your clients. Understanding that we need to keep certain joints mobile will solve a ton of your movement discrepancies on the field and in the gym.
If you’re feeling the squat or RDLs mostly in your back, there’s a reason! If you’re feeling the bench press predominantly in your anterior delts, there’s a reason! Give your mobility a check and get to work fixing your mobility problems so you can get the most out of your training, get out of pain, and stay on the field!